Policy context
In 2021, the World Health Organization (WHO) published new air quality guidelines, updating the 2005 air quality guidelines on the basis of a systematic review of the latest scientific evidence of how air pollution damages human health.
The European Union (EU) has also set standards for key air pollutants in the ambient air quality directives. Where levels exceed these standards, Member States should prepare an air quality plan or programme to address the sources responsible and ensure compliance. Although these values were based on the 2005 WHO air quality guidelines, they also reflect the technical and economic feasibility of their attainment across EU Member States. The EU air quality standards are therefore less demanding than the WHO air quality guidelines.
Under the European Green Deal’s Zero Pollution Action Plan, the European Commission set the 2030 goal of reducing the number of premature deaths caused by PM2.5 by at least 55% compared with 2005 levels. To this end, the European Commission initiated a revision of the ambient air quality directives, aiming to align the air quality standards more closely with WHO recommendations. The revision also aims to strengthen provisions on air quality monitoring and modelling, and on the development of air quality plans to help local authorities achieve cleaner air. In parallel, stricter requirements are also foreseen to tackle air pollution at source, such as from agriculture, industry, transport, buildings and energy.
This chapter directly supports the revision of EU air quality rules by providing a preliminary analysis of the health benefits of moving closer to WHO recommendations on air quality in the EU. It also assesses progress towards the Zero Pollution Action Plan target of reducing the health impacts of air pollution by more than 55% by 2030.
The new WHO air quality guidelines reflect concentrations of key air pollutants above which adverse health effects are known to occur. They offer quantitative health-based recommendations for air quality management and provide an evidence-based tool for policy makers working on air quality. The guidelines also include ‘interim targets’ — levels associated with a qualified reduction in the risk to health — that serve to inform the development of pollution reduction policies that are achievable in realistic timeframes in highly polluted areas. WHO recommends that the interim targets be regarded as steps towards the ultimate achievement of air quality guideline levels, rather than as an end goal.
Potential health benefits of achieving the EU limit values and WHO guideline levels for fine particulate matter
The EEA undertook a preliminary assessment of the potential benefits to human health — in terms of avoided premature deaths — of reducing fine particulate matter (PM2.5) air pollution across the EU to meet limit values established by the EU and guidelines set by WHO in 2021. Annual mean concentrations of PM2.5 in 2019 were taken as the point of departure and the following five standards and guideline levels were considered:
- EU limit value of 25 µg/m3
- EU indicative limit value of 20 µg/m3
- 2021 WHO interim target 3 of 15 µg/m3
- 2021 WHO interim target 4 of 10 µg/m3 (the 2005 WHO air quality guideline)
- 2021 WHO air quality guideline of 5 µg/m3
Table 1 describes the minimum health benefits that would have been achieved if, in 2019, all areas in the EU-27 had met the range of air quality concentrations for PM2.5 included in the EU standards and WHO guideline levels. It also shows the percentage change in relation to the situation in 2005, allowing for comparison with the target in the Zero Pollution Action Plan. Table 2 presents the minimum health benefits by country.
It is important to note that the assessment assumes that all areas in the EU-27 that were above each standard or guideline for PM2.5 in 2019, had instead reached each respective standard or guideline, while all other areas maintained the concentrations observed in 2019. As such, these estimates represent the minimum benefits that would result from improvements in air quality across the EU. The measures required to bring down concentrations in areas that were above a certain standard or guideline in 2019 would also reduce concentrations in areas already below the respective level, in particular for the WHO interim targets 3 and 4. Additional reductions in premature deaths would therefore also be seen in those areas and these benefits are not captured in this analysis, making it an underestimate of the potential health benefits.
|
EU-27
|
Premature deaths due to PM2.5
|
Reduction in premature deaths on 2019 levels
|
% reduction in premature deaths on 2019 levels
|
% reduction in premature deaths on 2005 levels
|
|
2019 concentrations
|
306,700
|
-
|
-
|
33%
|
|
EU limit value
25 µg/m3
|
306,500
|
200
|
0%
|
33%
|
|
EU indicative limit value
20 µg/m3
|
303,500
|
3,200
|
1%
|
33%
|
|
2021 WHO interim target 3
15 µg/m3
|
289,200
|
17,500
|
6%
|
37%
|
|
2021 WHO interim target 4
(2005 WHO air quality guideline)
10 µg/m3
|
241,400
|
65,300
|
21%
|
47%
|
|
2021 WHO air quality guideline
5 µg/m3
|
129,400
|
177,300
|
58%
|
72%
|
Note: The WHO interim targets and guidelines are drawn from the updated guidelines published in 2021.
Had the EU limit value for PM2.5 of 25 µg/m3 been attained across Europe in 2019, the estimated number of premature deaths would remain unchanged compared to the estimation with the 2019 real concentrations.
Had the EU indicative limit value of 20 µg/m3 been attained, only 1% fewer deaths would have been expected in the EU-27 and around 2% fewer across all 41 countries included in the analysis.
In contrast, had the WHO interim target 4 for PM2.5 of 10 µg/m3 been attained everywhere in Europe in 2019, premature deaths would have been at least 21% lower in the EU-27, and 22% lower across all 41 countries.
Finally, had the new WHO air quality guideline for PM2.5 of 5 µg/m3 been attained across Europe in 2019, the related premature deaths would have been 58% lower than in 2019 in both the EU-27 and all the European countries considered. Work is ongoing in the context of the revision of the EU ambient air quality directives to determine whether achieving PM2.5 concentrations of 5 µg/m3 is technically feasible across the EU, given the influence of geographical features in some areas.
Progress towards the Zero Pollution Action Plan target on air pollution
The Zero Pollution Action Plan sets the target of improving air quality, with a focus on PM2.5, in order to reduce the number of premature deaths caused by air pollution in the EU by a minimum of 55%, relative to 2005 levels. The EEA estimates that 456,000 premature deaths were attributable to exposure to PM2.5 in 2005 in the 27 Member States of the EU. Achieving a 55% reduction would imply that premature deaths fell to 205,000 per year.
In terms of the past trend, from 2005 to 2019 premature deaths attributed to PM2.5 exposure in the EU 27 fell by 33% to reach 307,000 (see Figure 1). Should air quality continue to improve, and the number of premature deaths per year continue to fall at a comparable rate in the future, then the target would be achieved by 2032, as shown in Figure 1. However, continuously reducing concentrations of particulate matter in ambient air over the next decade will be demanding. To meet the target, Member States will need to fully implement their national air pollution control programmes (NACPCs), as well as measures needed to reach the 2030 climate and energy targets (European Commission, 2021). Furthermore, the trends in aging and urbanisation of the European population counteract some of the health gains associated with the reduction in ambient air pollution concentrations. An older population is more sensitive to air pollution and a higher rate of urbanisation typically means that more people are exposed to PM2.5 concentrations, which tend to be higher in cities.
Note: To estimate premature deaths, all-cause (natural) mortality is considered in people aged over 30 years for all concentrations, assuming a linear increase in the risk of mortality of 6.2% for a 10 μg/m3 increase in concentrations of PM2.5
The trend in premature deaths is based on a future projection of the past rate of reduction in premature deaths.
Source: ETC/ATNI, 2021
More info here...
The analysis of the potential benefits of meeting different EU limit values and WHO guideline levels indicates that the target to reduce premature deaths by 55% can only be met by lowering concentrations of PM2.5 across the EU to levels comparable to the 2021 WHO air quality guideline.
Had the WHO interim target 4 for PM2.5 of 10 µg/m3 (the 2005 WHO air quality guideline) been attained across the EU-27 in 2019, this would have delivered a reduction in premature deaths of at least 47% on 2005 levels (see Figure 2 and Table 1). This would not have been sufficient to meet the Zero Pollution Action Plan target in full in 2019, although it is important to note that this does not capture the benefits of reducing pollution in areas that were already at 10 µg/m3 or less in 2019.
However, had the new WHO air quality guideline for PM2.5 of 5 µg/m3 been attained across the EU-27 in 2019, then this would have delivered a reduction in premature deaths of at least 72% compared with 2005 levels (see figure 2).
Bringing PM2.5 concentrations closer to the 2021 WHO air quality guideline would therefore deliver significant health benefits in Europe. EU air quality standards are a crucial policy tool driving improvements in air quality. The closer alignment of EU air quality standards with WHO recommendations would therefore represent an important step towards cleaner air in Europe.
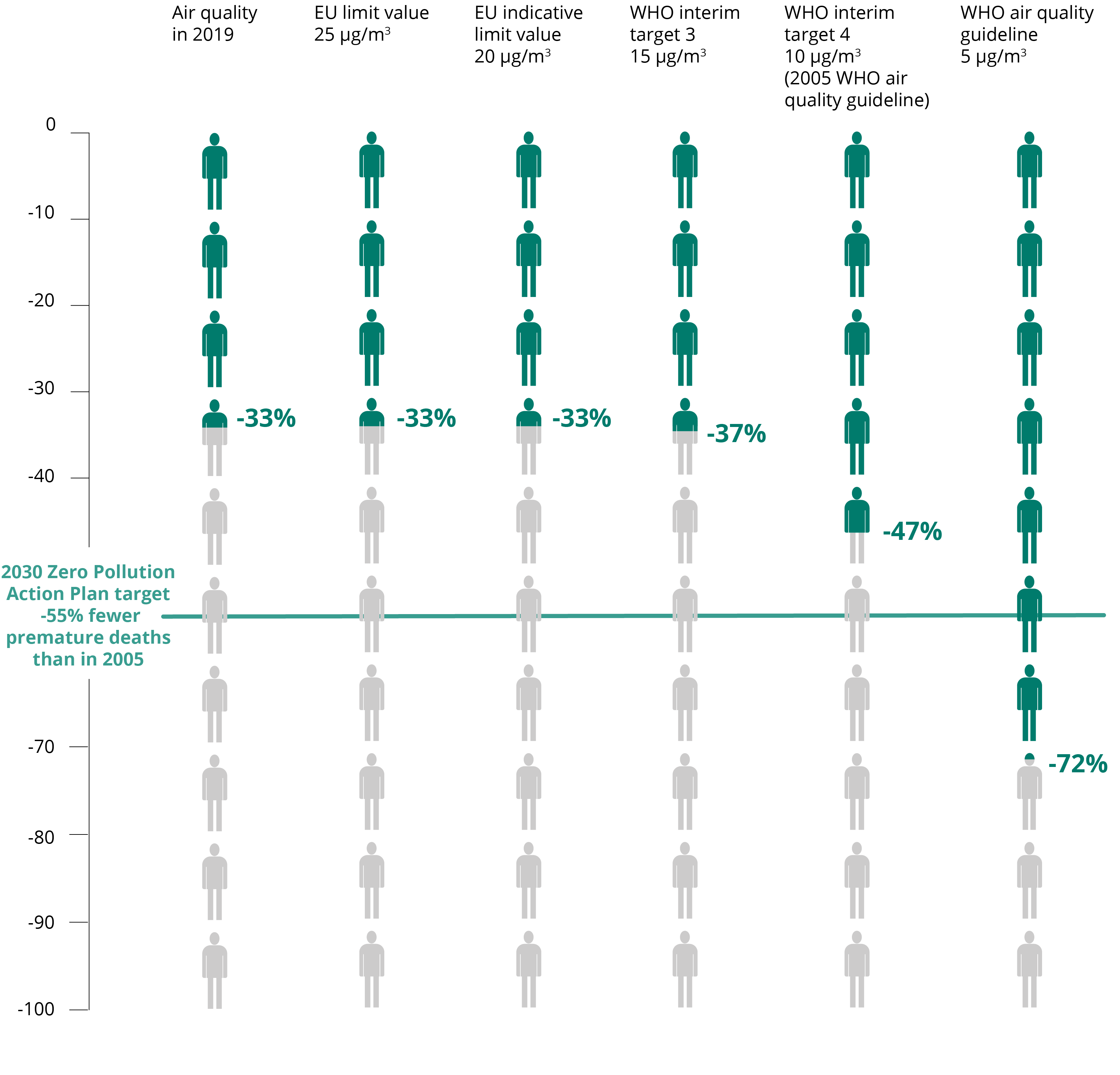
Note: The graph presents the estimated minimum reduction in premature deaths due to exposure to PM2.5 compared with 2005, had different EU limit values and WHO guidelines for PM2.5 been met in the EU-27 in 2019.
Health impacts of air pollution in Europe in 2019
Estimations of the mortality in 2019 linked to exposure to the air pollutants deemed most harmful for human health are presented in this final section.
In 2019 in the EU-27:
- 307,000 premature deaths were attributed to exposure to PM2.5
- 40,400 premature deaths were attributed to exposure to nitrogen dioxide (NO2)
- 16,800 premature deaths were attributed to exposure to ozone (O3)
In 2019 in the 41 European countries considered:
- 373,000 premature deaths were attributed to exposure to PM2.5
- 47,700 premature deaths were attributed to exposure to NO2
- 19,070 premature deaths were attributed to exposure to O3
The number of premature deaths attributed to air pollution fell in 2019 compared to 2018. The greatest decrease was for NO2, with a reduction of 16% in the associated premature deaths. Premature deaths attributed to exposure to fine particulate matter decreased by 11%, while those attributed to exposure to ozone decreased by 9%.
Table 3 presents the total country population, the population-weighted mean concentrations, and the estimated number of attributable premature deaths by country.
Table 4 presents years of life lost (YLL), and the YLL per 100,000 inhabitants associated with exposure to PM2.5, NO2 and O3 concentration levels in 2019.
The sections below provide information at country level on the health impacts of key pollutants. For specific information on the pollutants, concentrations and their sources, please see the chapter on Europe’s air quality status 2021 - update.
Additional information on the data and the methodology used can be found in the Eionet ETC/ATNI report 10/2021, Health risk assessments of air pollution.
The greatest health risks in terms of premature deaths and years of life lost (YLL) attributable to PM2.5 exposure are estimated for the countries with some of the largest populations, namely, in order of decreasing rank, Germany, Italy, Poland, the United Kingdom and France.
However, when considering YLL per 100,000 inhabitants, the most significant impacts are observed in central and eastern European countries (where the highest concentrations of PM2.5 are also observed), namely, in order of decreasing rank, Bosnia and Herzegovina, Serbia, Kosovo, North Macedonia and Bulgaria. The smallest relative impacts are found in countries situated in the north and north-west of Europe, where concentrations are lowest.
The greatest health risks in terms of premature deaths and years of life lost (YLL) attributable to NO2 exposure are estimated for the countries with some of the largest populations, namely, in order of decreasing rank, Italy, Spain, Germany, the United Kingdom and France.
When considering YLL per 100,000 inhabitants, the most significant impacts are observed in, in order of decreasing rank, Greece, Romania, Italy, Bulgaria and Spain. The smallest relative impacts on health are found in the Nordic and Baltic countries.
The greatest health risks in terms of total premature deaths and years of life lost (YLL) attributable to O3 exposure were seen for, in order of decreasing rank, Germany, Italy, France, Spain and Poland.
The countries with the highest rates of YLL per 100,000 inhabitants were, in order of decreasing rank, Bosnia and Herzegovina, Montenegro, Albania, Croatia and Greece. The countries with the lowest relative impacts on health from O3 exposure were, in order of increasing rank, Iceland, Ireland, the United Kingdom, Norway and Finland.
Estimating the health risks of air pollution
Since 2014, the EEA has been estimating mortality due to exposure to air pollution, with support from the EEA European Topic Centres. Mortality is both the most serious health outcome of air pollution, and also the one for which scientific evidence is most robust. To attribute a health risk to exposure to air pollution, concentration-response functions are used. These functions are based on epidemiological studies and estimate the increase in risk per unit of concentration of a certain air pollutant. As an example, the function for fine particles (PM2.5) assumes a linear increase in the risk of mortality of 6.2% for a 10 µg/m3 increase in PM2.5.
To date, the EEA has used the risks functions recommended by WHO in 2013. To ensure comparability with our previous studies, the same 2013 functions are used in this chapter. The new 2021 WHO air quality guidelines include new concentration-response functions and the EEA expects to apply these new functions in our assessments from 2022 onwards.
Note 1: The analysis in this chapter refers to the 27 Member States of the European Union (EU-27), as well as additional European countries, reaching a total of 41 countries.
The quantifications of health risks are done individually for the respective air pollutants, and they cannot be added together, as they exhibit some degree of correlation.
Note 2: Our assessment of potential benefits assumes that all areas in the EU-27 that in 2019 were above each respective standard or guideline for PM2.5 had instead reached each respective standard or guideline, while all other areas maintained the concentrations observed in 2019. As such, these estimates represent the minimum benefits resulting from potential improvements in air quality across the EU, with reductions in premature deaths also likely to be seen in areas where standards and guidelines were already achieved.
Note 3: The withdrawal of the United Kingdom from the European Union did not affect the production of this assessment. Data for the United Kingdom appear here in agreement with the terms of the Withdrawal Agreement, which entered into force on 1 February 2020. Data reported by the United Kingdom are included in all analyses and assessments contained herein, unless otherwise indicated.
Chapters of the Air quality in Europe 2021 report:

How clean is the air you are breathing right now? Check the Air quality index for desktop, here.

Download the Air quality index app for Android or iPhone/iPad, by scanning the QR code with your phone.
Identifiers
Briefing no. 19/2021
Title: Health impacts of air pollution in Europe, 2021
HTML - TH-AM-21-012-EN-Q - ISBN 978-92-9480-404-4 - ISSN 2467-3196 - doi: 10.2800/08097

Document Actions
Share with others